Asthma - children
Pediatric asthma; Asthma - pediatric; Wheezing - asthma - children
Asthma is a disease that causes the airways to swell and get narrow. It leads to wheezing, shortness of breath, chest tightness, and coughing.
Asthma
Asthma is a disease that causes the airways of the lungs to swell and narrow. It leads to wheezing, shortness of breath, chest tightness, and coughi...

Causes
Asthma is caused by swelling (inflammation) in the airways. During an asthma attack, the muscles surrounding the airways tighten. The lining of the air passages swells. Less air is able to pass through as a result.
Asthma is often seen in children. It is a leading cause of missed school days and hospital visits for children. An allergic reaction is a key part of asthma in children. Asthma and allergies often occur together.
Asthma and allergies
The following organizations are good resources for information on asthma and allergies:Allergy and Asthma Network -- www. allergyasthmanetwork. orgAm...
In children who have sensitive airways, asthma symptoms can be triggered by breathing in substances called allergens or triggers .
Allergens
An allergen is a substance that can cause an allergic reaction. In some people, the immune system recognizes allergens as foreign or dangerous. As ...

Triggers
Asthma triggers - stay away from; Asthma triggers - avoiding; Reactive airway disease - triggers; Bronchial asthma - triggers

Common asthma triggers include:
- Animals (hair or dander)
- Dust, mold, and pollen
- Aspirin and other medicines
- Changes in weather (most often cold weather)
- Chemicals in the air or in food
- Tobacco smoke
- Exercise
- Strong emotions
- Viral infections, such as the common cold
Symptoms
Breathing problems are common. They can include:
- Shortness of breath
- Feeling out of breath
- Gasping for air
- Trouble breathing out (exhaling)
- Breathing faster than normal
When the child is having a hard time breathing, the skin of the chest and neck may suck inward.
Other symptoms of asthma in children include:
- Coughing that sometimes wakes the child up at night (it may be the only symptom).
- Dark bags under the eyes.
- Feeling tired.
- Irritability.
- Tightness in the chest.
-
A whistling sound made when breathing (
wheezing
). You may notice it more when the child breathes out.
Wheezing
Wheezing is a high-pitched whistling sound during breathing. It occurs when air moves through narrowed breathing tubes in the lungs.
ImageRead Article Now Book Mark Article
Your child's asthma symptoms may vary. Symptoms may appear often or develop only when triggers are present. Some children are more likely to have asthma symptoms at night.
Exams and Tests
The health care provider will use a stethoscope to listen to the child's lungs. The provider may be able to hear asthma sounds. However, lung sounds are often normal when the child is not having an asthma episode .
Asthma episode
Asthma attack - signs of; Reactive airway disease - asthma attack; Bronchial asthma - attack
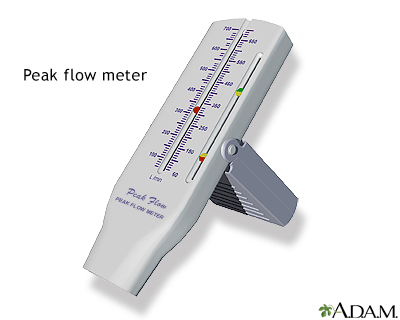
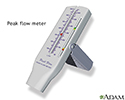
The provider will have the child breathe into a device called a peak flow meter . Peak flow meters can tell how well the child can blow air out of the lungs. If the airways are narrow due to asthma, peak flow values drop.
Peak flow meter
Peak flow meter - how to use; Asthma - peak flow meter; Reactive airway disease - peak flow meter; Bronchial asthma - peak flow meter

You and your child will learn to measure peak flow at home.
Tests may include:
-
Allergy testing on the
skin
, or a
blood test
to see if your child is allergic to certain substances
Skin
Allergy skin tests are used to find out which substances cause a person to have an allergic reaction.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleBlood test
An absolute eosinophil count is a blood test that measures the number of white blood cells called eosinophils. Eosinophils become active when you ha...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Chest x-ray
Chest x-ray
A chest x-ray is an x-ray of the chest, lungs, heart, large arteries, ribs, and diaphragm.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Lung function tests
Lung function tests
Pulmonary function tests are a group of tests that measure breathing and how well the lungs are functioning.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
You and your child's providers should work together as a team to create and carry out an asthma action plan.
This plan will tell you how to:
-
Avoid asthma triggers
Avoid asthma triggers
Asthma triggers - stay away from; Asthma triggers - avoiding; Reactive airway disease - triggers; Bronchial asthma - triggers
ImageRead Article Now Book Mark Article -
Monitor symptoms
Monitor symptoms
Asthma attack - signs of; Reactive airway disease - asthma attack; Bronchial asthma - attack
Read Article Now Book Mark Article - Measure peak flow
- Take medicines
The plan should also tell you when to call the provider. It is important to know what questions to ask your child's provider .
Questions to ask your child's provider
What to ask your doctor about asthma - child
Children with asthma need a lot of support at school .
Support at school
Asthma action plan - school; Wheezing - school; Reactive airway disease - school; Bronchial asthma - school
- Give the school staff your asthma action plan so they know how to take care of your child's asthma.
- Find out how to let your child take medicine during school hours. (You may need to sign a consent form.)
-
Having asthma does not mean your child cannot exercise. Coaches, gym teachers, and your child should know what to do if your child has asthma
symptoms caused by exercise
.
Symptoms caused by exercise
Asthma - exercise school; Exercise - induced asthma - school
Read Article Now Book Mark Article
ASTHMA MEDICINES
There are two basic kinds of medicine used to treat asthma.
Long-term control drugs are taken every day to prevent asthma symptoms. Your child should take these medicines even if no symptoms are present. Some children may need more than one long-term control medicine.
Types of long-term control medicines include:
Control medicines
Asthma - inhaled corticosteroids; Asthma - long-acting beta-agonists; Asthma - leukotriene modifiers; Asthma - cromolyn; Bronchial asthma-control dru...

- Inhaled steroids (these are usually the first choice of treatment)
- Long-acting bronchodilators (these are almost always used with inhaled steroids)
- Leukotriene inhibitors
- Cromolyn sodium
Quick relief or rescue asthma drugs work fast to control asthma symptoms. Children take them when they are coughing, wheezing, having trouble breathing, or having an asthma attack.
Quick relief
Asthma - quick-relief drugs - short-acting beta-agonists; Asthma - quick-relief drugs - bronchodilators; Asthma - quick-relief drugs - oral steroids;...

Some of your child's asthma medicines can be taken using an inhaler .
Inhaler
Metered-dose inhaler (MDI) administration - no spacer; Bronchial nebulizer; Wheezing - nebulizer; Reactive airway - nebulizer; COPD - nebulizer; Chro...

-
Children who use an inhaler should use a
spacer device
. This helps them get the medicine into the lungs properly.
Spacer device
Metered-dose inhaler (MDI) administration - with spacer; Asthma - inhaler with spacer; Reactive airway disease - inhaler with spacer; Bronchial asthm...
Read Article Now Book Mark Article - If your child uses the inhaler the wrong way, less medicine gets into the lungs. Have your provider show your child how to correctly use an inhaler.
-
Younger children can use a
nebulizer
instead of an inhaler to take their medicine. A nebulizer turns asthma medicine into a mist.
Nebulizer
Nebulizer - how to use; Asthma - how to use a nebulizer; COPD - how to use a nebulizer; Wheezing - nebulizer; Reactive airway - nebulizer; COPD - neb...
Read Article Now Book Mark Article
GETTING RID OF TRIGGERS
It is important to know your child's asthma triggers. Avoiding them is the first step toward helping your child feel better.
Keep pets outdoors, or at least away from the child's bedroom.
No one should smoke in a house or around a child with asthma.
- Getting rid of tobacco smoke in the home is the single most important thing a family can do to help a child with asthma.
- Smoking outside the house is not enough. Family members and visitors who smoke carry the smoke inside on their clothes and hair. This can trigger asthma symptoms.
- DO NOT use indoor fireplaces.
Keep the house clean. Keep food in containers and out of bedrooms. This helps reduce the possibility of cockroaches, which can trigger asthma attacks. Cleaning products in the home should be unscented.
MONITOR YOUR CHILD'S ASTHMA
Checking peak flow is one of the best ways to control asthma. It can help you keep your child's asthma from getting worse. Asthma attacks usually DO NOT happen without warning.
Children under age 5 may not be able to use a peak flow meter well enough for it to be helpful. However, a child should start using the peak flow meter at a young age to get used to it. An adult should always watch for a child's asthma symptoms.
Use a peak flow meter
Peak flow meter - how to use; Asthma - peak flow meter; Reactive airway disease - peak flow meter; Bronchial asthma - peak flow meter
Outlook (Prognosis)
With proper treatment, most children with asthma can live a normal life. When asthma is not well controlled, it can lead to missed school, problems playing sports, missed work for parents, and many visits to the doctor's office and emergency room.
Asthma symptoms often lessen or go away completely as the child gets older. Asthma that is not well controlled can lead to lasting lung problems.
In rare cases, asthma is a life-threatening disease. Families need to work closely with their providers to develop a plan to care for a child with asthma.
When to Contact a Medical Professional
Call your child's provider if you think your child has new symptoms of asthma. If your child has been diagnosed with asthma, call the provider:
- After an emergency room visit
- When peak flow numbers have been getting lower
- When symptoms get more frequent and more severe, even though your child is following the asthma action plan
If your child is having trouble breathing or having an asthma attack, get medical help right away.
Emergency symptoms include:
Emergency symptoms
Asthma attack - signs of; Reactive airway disease - asthma attack; Bronchial asthma - attack
- Difficulty breathing
- Bluish color to the lips and face
- Severe anxiety due to shortness of breath
- Rapid pulse
- Sweating
- Decreased level of alertness, such as severe drowsiness or confusion
A child who is having a severe asthma attack may need to stay in the hospital and get oxygen and medicines through a vein (intravenous line or IV).
References
Jackson DJ, Lemanske RF, Guilbert TW. Management of asthma in infants and children. In: Adkinson NF, Bochner BS, Burks AW, et al, eds. Middleton's Allergy Principles and Practice . 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:chap 53.
Lugogo N, Que LG, Gilstrap DL, Kraft M. Asthma: clinical diagnosis and management. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel's Textbook of Respiratory Medicine . 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 42.
National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Rockville, MD. National Heart, Lung, and Blood Institute, US Dept of Health and Human Services; 2007. NIH publications 08-4051. Updated April 2012. www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm . Accessed June 10, 2015.
-
Asthma - children
Animation
-
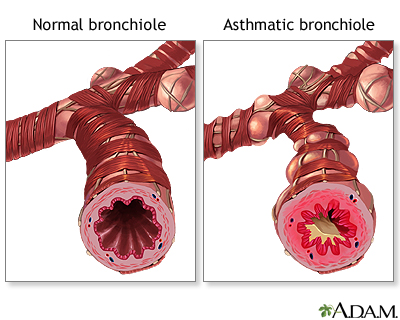
Normal versus asthmatic bronchiole - illustration
During an asthma attack smooth muscles located in the bronchioles of the lung constrict and decrease the flow of air in the airways. The amount of air flow can further be decreased by inflammation or excess mucus secretion.
Normal versus asthmatic bronchiole
illustration
-
Peak flow meter - illustration
A peak flow meter is commonly used by a person with asthma to measure the amount of air that can be expelled from the lungs. If the airways become narrow or blocked due to asthma, peak flow values will drop because the person cannot blow air out of the lungs as well. A peak flow meter can be a useful aid in monitoring a person's asthma over time and can also be used to help determine how well a patient's medications are working.
Peak flow meter
illustration
-
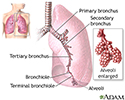
Lungs - illustration
The major features of the lungs include the bronchi, the bronchioles and the alveoli. The alveoli are the microscopic blood vessel-lined sacks in which oxygen and carbon dioxide gas are exchanged.
Lungs
illustration
-
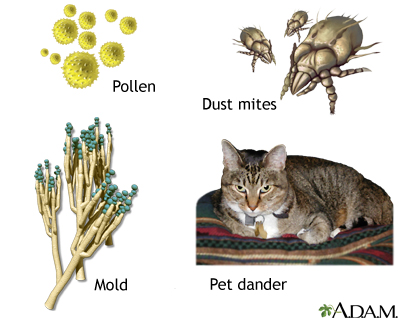
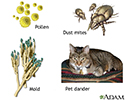
Common asthma triggers - illustration
Many of the same substances that trigger allergies can also trigger asthma. Common allergens include pollen, dust mites, mold and pet dander. Other asthma triggers include irritants like smoke, pollution, fumes, cleaning chemicals, and sprays. Asthma symptoms can be substantially reduced by avoiding exposure to known allergens and respiratory irritants.
Common asthma triggers
illustration

-
Normal versus asthmatic bronchiole - illustration
During an asthma attack smooth muscles located in the bronchioles of the lung constrict and decrease the flow of air in the airways. The amount of air flow can further be decreased by inflammation or excess mucus secretion.
Normal versus asthmatic bronchiole
illustration
-
Peak flow meter - illustration
A peak flow meter is commonly used by a person with asthma to measure the amount of air that can be expelled from the lungs. If the airways become narrow or blocked due to asthma, peak flow values will drop because the person cannot blow air out of the lungs as well. A peak flow meter can be a useful aid in monitoring a person's asthma over time and can also be used to help determine how well a patient's medications are working.
Peak flow meter
illustration
-
Lungs - illustration
The major features of the lungs include the bronchi, the bronchioles and the alveoli. The alveoli are the microscopic blood vessel-lined sacks in which oxygen and carbon dioxide gas are exchanged.
Lungs
illustration
-
Common asthma triggers - illustration
Many of the same substances that trigger allergies can also trigger asthma. Common allergens include pollen, dust mites, mold and pet dander. Other asthma triggers include irritants like smoke, pollution, fumes, cleaning chemicals, and sprays. Asthma symptoms can be substantially reduced by avoiding exposure to known allergens and respiratory irritants.
Common asthma triggers
illustration
Review Date: 4/21/2015
Reviewed By: Neil K. Kaneshiro, MD, MHA, Clinical Assistant Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Internal review and update on 07/24/2016 by David Zieve, MD, MHA, Isla Ogilvie, PhD, and the A.D.A.M. Editorial team.