Endocardial cushion defect
Atrioventricular (AV) canal defect; Atrioventricular septal defect; AVSD; Common AV orifice; Ostium primum atrial septal defects; Congenital heart defect - ECD; Birth defect - ECD; Cyanotic disease - ECD
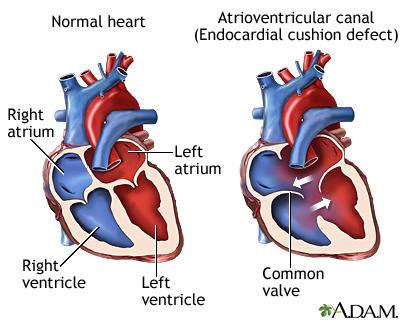
Endocardial cushion defect (ECD) is an abnormal heart condition. The walls separating all 4 chambers of the heart are poorly formed or absent. Also, the valves separating the upper and lower chambers of the heart have defects during formation. ECD is a congenital heart disease , which means it is present from birth.
Congenital heart disease
Congenital heart disease (CHD) is a problem with the heart's structure and function that is present at birth.

Causes
ECD occurs while a baby is still growing in the womb. The endocardial cushions are two thicker areas that develop into the walls (septum) that divide the 4 chambers of the heart. They also form the mitral and tricuspid valves. These are the valves that separate the atria (top collecting chambers) from the ventricles (bottom pumping chambers).
The lack of separation between the two sides of the heart causes several problems:
- Increased blood flow to the lungs. This results in increased pressure in the lungs. In ECD, blood flows through the abnormal openings from the left to the right side of the heart, then to the lungs. More blood flow into the lungs makes the blood pressure in the lungs rise.
-
Heart failure
. The extra effort needed to pump makes the heart work harder than normal. The heart muscle may enlarge and weaken. This can cause swelling in the baby, problems in breathing, and difficulty in feeding and growing.
Heart failure
Heart failure is a condition in which the heart is no longer able to pump oxygen-rich blood to the rest of the body efficiently. This causes symptom...
ImageRead Article Now Book Mark Article -
Cyanosis
. As the blood pressure increases in the lungs, blood starts to flow from the right side of the heart to the left. The oxygen-poor blood mixes with the oxygen-rich blood. As a result, blood with less oxygen than usual is pumped out to the body. This causes cyanosis, or bluish skin.
Cyanosis
Cyanosis is a bluish color to the skin or mucous membrane that is usually due to a lack of oxygen in the blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
There are two types of ECD:
- Complete ECD. This condition involves an atrial septal defect (ASD) and a ventricular septal defect (VSD). People with a complete ECD have only one large heart valve (common AV valve) instead of two distinct valves (mitral and tricuspid).
- Partial (or incomplete) ECD. In this condition, only an ASD, or an ASD and VSD are present. There are two distinct valves, but one of them (the mitral valve) is often abnormal with an opening ("cleft") in it. This defect can leak blood back through the valve.
ECD is strongly linked to Down syndrome . Several gene changes are also linked to ECD. However, the exact cause of ECD is unknown.
Down syndrome
Down syndrome is a genetic condition in which a person has 47 chromosomes instead of the usual 46.
ECD may be associated with other congenital heart defects, such as:
-
Double outlet right ventricle
Double outlet right ventricle
Double outlet right ventricle (DORV) is a heart disease that is present from birth (congenital). The aorta connects to the right ventricle (RV, the ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Single ventricle
-
Transposition of the great vessels
Transposition of the great vessels
Transposition of the great vessels is a heart defect that occurs from birth (congenital). The 2 major vessels that carry blood away from the heart -...
ImageRead Article Now Book Mark Article -
Tetralogy of Fallot
Tetralogy of Fallot
Tetralogy of Fallot is a type of congenital heart defect. Congenital means that it is present at birth.
ImageRead Article Now Book Mark Article
Symptoms
Symptoms of ECD may include:
- Baby tires easily
- Bluish skin color, also known as cyanosis (the lips may also be blue)
- Feeding difficulties
- Failure to gain weight and grow
- Frequent pneumonia or infections
- Pale skin (pallor)
-
Rapid breathing
Rapid breathing
Transient tachypnea is a breathing disorder seen shortly after delivery in full-term or late preterm babies. Transient means it is short-lived (most ...
Read Article Now Book Mark Article - Rapid heartbeat
- Sweating
- Swollen legs or abdomen (rare in children)
- Trouble breathing, especially during feeding
Exams and Tests
During an exam, the health care provider will likely find signs of ECD, including:
- An abnormal electrocardiogram (ECG)
- An enlarged heart
- Heart murmur
Children with partial ECD may not have signs or symptoms of the disorder during childhood.
Tests to diagnose ECD include:
-
Echocardiogram
, which is an ultrasound that views the heart structures and blood flow inside the heart
Echocardiogram
An echocardiogram is a test that uses sound waves to create pictures of the heart. The picture and information it produces is more detailed than a s...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Electrocardiogram (
ECG
), which measures the electrical activity of the heart
ECG
An electrocardiogram (ECG) is a test that records the electrical activity of the heart.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Chest x-ray
Chest x-ray
A chest x-ray is an x-ray of the chest, lungs, heart, large arteries, ribs, and diaphragm.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
MRI
, which provides a detailed image of the heart
MRI
A magnetic resonance imaging (MRI) scan is an imaging test that uses powerful magnets and radio waves to create pictures of the body. It does not us...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Cardiac catheterization
, a procedure in which a thin tube (catheter) is placed into the heart to see blood flow and take accurate measurements of blood pressure and oxygen levels
Cardiac catheterization
Cardiac catheterization involves passing a thin flexible tube (catheter) into the right or left side of the heart. The catheter is most often insert...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
Surgery is needed to close the holes between the heart chambers, and to create distinct tricuspid and mitral valves. The timing of the surgery depends on the child's condition and the severity of the ECD. It can often be done when the baby is 3 to 6 months old. Correcting an ECD may require more than one surgery.
Your child's doctor may prescribe medicine:
- To treat the symptoms of heart failure
- Before surgery if ECD has made your baby very sick
The medicines will help your child gain weight and strength before surgery. Medicines often used include:
- Diuretics (water pills)
- Drugs that make the heart contract more forcefully, such as digoxin
Surgery for a complete ECD should be done in the baby's first year of life. Otherwise, lung damage that may not be able to be reversed can occur. Babies with Down syndrome tend to develop lung disease earlier. Therefore, early surgery is very important for these babies.
Outlook (Prognosis)
How well your baby does depends on:
- The severity of the ECD
- The child's overall health
- Whether lung disease has already developed
Many children live normal, active lives after ECD is corrected.
Possible Complications
Complications from ECD may include:
-
Congestive heart failure
Congestive heart failure
Heart failure is a condition in which the heart is no longer able to pump oxygen-rich blood to the rest of the body efficiently. This causes symptom...
ImageRead Article Now Book Mark Article - Death
-
Eisenmenger syndrome
Eisenmenger syndrome
Eisenmenger syndrome is a condition that affects blood flow from the heart to the lungs in some people who were born with structural problems of the ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - High blood pressure in the lungs
- Irreversible damage to the lungs
Certain complications of ECD surgery may not appear until the child is an adult. These include heart rhythm problems and a leaky mitral valve.
Children with ECD may be at risk for infection of the heart ( endocarditis ) before and after surgery. Ask your child's doctor whether your child needs to take antibiotics before certain dental procedures.
Endocarditis
Endocarditis is inflammation of the inside lining of the heart chambers and heart valves (endocardium). It is caused by a bacterial or, rarely a fun...
When to Contact a Medical Professional
Call your child's provider if your child:
- Tires easily
- Has trouble breathing
- Has bluish skin or lips
Also talk to the provider if your baby is not growing or gaining weight.
Prevention
ECD is linked with several genetic abnormalities. Couples with a family history of ECD may wish to seek genetic counseling before becoming pregnant.
References
Bope ET, Kellerman RD. The cardiovascular system. In: Bope ET, Kellerman RD, eds. Conn's Current Therapy 2016 . Philadelphia, PA: Elsevier; 2016:chap 7.
Kliegman RM, Stanton BF, St. Geme JW, Schor NF. Acyanotic congenital heart disease. In: Kliegman RM, Stanton BF, St. Geme JW, Schor NF, eds. Nelson Textbook of Pediatrics . 20th ed. Philadelphia, PA: Elsevier; 2016:chap 426.
Kouchoukos NT, Blackstone EH, Hanley FL, Kirklin JK. Atrioventricular septal defect. In: Kouchoukos NT, Blackstone EH, Hanley FL, Kirklin JK, eds. Kirklin/Barratt-Boyes Cardiac Surgery . 4th ed. Philadelphia, PA: Elsevier Saunders; 2013:chap 34.
Robinson JD, Rigsby CK, Thakrar D. Septal defects. In: Coley BD, ed. Caffey's Pediatric Diagnostic Imaging . 12th ed. Philadelphia, PA: Elsevier Saunders; 2013:chap 73.
-
Congenital heart defect overview
Animation
-
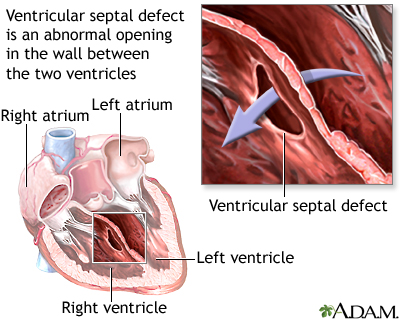
Ventricular septal defect - illustration
Ventricular septal defect is a congenital defect of the heart, that occurs as an abnormal opening in the wall that separates the right and left ventricles. Ventricular septal defect may also be associated with other heart defects. Many small defects will close on their own. For those defects that do not spontaneously close, the outcome is good with surgical repair.
Ventricular septal defect
illustration
-
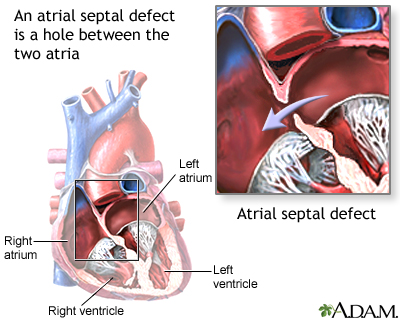
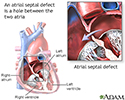
Atrial septal defect - illustration
An atrial septal defect is a congenital heart defect where the wall between the right and left atria does not close properly, leaving a hole between the two atria.
Atrial septal defect
illustration
-
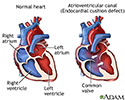
Atrioventricular canal (endocardial cushion defect) - illustration
Endocardial cushion defect is an abnormal heart condition which occurs during the development of the baby. In this condition there is no separation between the chambers of the heart. Without the separation, oxygen-rich and oxygen-poor blood mix causing the heart to work harder. Endocardial cushion defect is strongly associated with several genetic abnormalities.
Atrioventricular canal (endocardial cushion defect)
illustration

-
Ventricular septal defect - illustration
Ventricular septal defect is a congenital defect of the heart, that occurs as an abnormal opening in the wall that separates the right and left ventricles. Ventricular septal defect may also be associated with other heart defects. Many small defects will close on their own. For those defects that do not spontaneously close, the outcome is good with surgical repair.
Ventricular septal defect
illustration
-
Atrial septal defect - illustration
An atrial septal defect is a congenital heart defect where the wall between the right and left atria does not close properly, leaving a hole between the two atria.
Atrial septal defect
illustration
-
Atrioventricular canal (endocardial cushion defect) - illustration
Endocardial cushion defect is an abnormal heart condition which occurs during the development of the baby. In this condition there is no separation between the chambers of the heart. Without the separation, oxygen-rich and oxygen-poor blood mix causing the heart to work harder. Endocardial cushion defect is strongly associated with several genetic abnormalities.
Atrioventricular canal (endocardial cushion defect)
illustration
Review Date: 5/6/2016
Reviewed By: Scott I. Aydin, MD, Assistant Professor of Pediatrics, Albert Einstein College of Medicine, Division of Pediatric Cardiology and Critical Care Medicine, The Children's Hospital at Montefiore, Bronx, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Isla Ogilvie, PhD, and the A.D.A.M. Editorial team.