Acute tubular necrosis
Necrosis - renal tubular; ATN; Necrosis - acute tubular
Acute tubular necrosis is a kidney disorder involving damage to the tubule cells of the kidneys, which can lead to acute kidney failure .
Acute kidney failure
Acute kidney failure is the rapid (less than 2 days) loss of your kidneys' ability to remove waste and help balance fluids and electrolytes in your b...

Causes
Acute tubular necrosis (ATN) is often caused by a lack of blood flow and oxygen to the kidney tissues (ischemia of the kidneys). It may also occur if the kidney cells are damaged by a poison or harmful substance.
The internal structures of the kidney, particularly the tissues of the kidney tubule, become damaged or destroyed. ATN is one of the most common structural changes that can lead to acute renal failure.
ATN is a common cause of kidney failure in hospitalized people. Risks for ATN include:
-
Blood transfusion reaction
Blood transfusion reaction
A hemolytic transfusion reaction is a serious complication that can occur after a blood transfusion. The reaction occurs when the red blood cells th...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Injury or trauma that damages the muscles
- Low blood pressure (hypotension) that lasts longer than 30 minutes
- Recent major surgery
-
Septic shock
due to severe infection
Septic shock
Septic shock is a serious condition that occurs when a body-wide infection leads to dangerously low blood pressure.
Read Article Now Book Mark Article
Liver disease and kidney damage caused by diabetes ( diabetic nephropathy ) may make a person more susceptible to the condition.
Diabetic nephropathy
Kidney disease or kidney damage often occurs over time in people with diabetes. This type of kidney disease is called diabetic nephropathy.

ATN can also be caused by:
- Dye (contrast) used for x-ray (radiology) studies
- Medicines that are toxic to the kidneys (such as aminoglycoside antibiotics or amphotericin)
Symptoms
Symptoms may include any of the following:
-
Decreased consciousness
, coma,
delirium
or
confusion
, drowsiness, and lethargy
Decreased consciousness
Decreased alertness is a state of reduced awareness. A coma is a state of decreased alertness from which a person cannot be awakened. A long-term co...
Read Article Now Book Mark ArticleDelirium
Delirium is sudden severe confusion due to rapid changes in brain function that occur with physical or mental illness.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleConfusion
Confusion is the inability to think as clearly or quickly as you normally do. You may feel disoriented and have difficulty paying attention, remembe...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Decreased urine output
or no urine output
Decreased urine output
Decreased urine output means that you produce less urine than normal. Most adults make at least 500 ml of urine in 24 hours (a little over 2 cups)....
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - General swelling, fluid retention
- Nausea, vomiting
Exams and Tests
The health care provider will perform a physical exam. The provider may hear abnormal sounds when listening to the heart and lungs with a stethoscope ( auscultation ). This is due to too much fluid in the body.
Auscultation
Auscultation is listening to the sounds of the body during a physical examination.

Tests that may be done include:
-
BUN
and serum creatinine
BUN
BUN stands for blood urea nitrogen. Urea nitrogen is what forms when protein breaks down. A test can be done to measure the amount of urea nitrogen ...
Read Article Now Book Mark Article -
Fractional excretion of sodium
Fractional excretion of sodium
Fractional excretion of sodium is the amount of salt (sodium) that leaves the body through urine compared to the amount filtered and reabsorbed by th...
ImageRead Article Now Book Mark Article -
Kidney biopsy
Kidney biopsy
A kidney biopsy is the removal of a small piece of kidney tissue for examination.
ImageRead Article Now Book Mark Article -
Urinalysis
Urinalysis
Urinalysis is the physical, chemical, and microscopic examination of urine. It involves a number of tests to detect and measure various compounds th...
ImageRead Article Now Book Mark Article -
Urine sodium
Urine sodium
The sodium urine test measures the amount of sodium in a certain amount of urine. Sodium can also be measured in a blood sample.
ImageRead Article Now Book Mark Article -
Urine specific gravity
and
osmolarity urine
Urine specific gravity
Urine specific gravity is a laboratory test that shows the concentration of all chemical particles in the urine.
ImageRead Article Now Book Mark ArticleOsmolarity urine
The osmolality urine test measures the concentration of particles in urine. Osmolality can also be measured using a blood test.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
In most people, ATN is reversible. The goal of treatment is to prevent life-threatening complications of acute kidney failure
Treatment focuses on preventing the buildup of fluids and wastes, while allowing the kidneys to heal.
Treatment may include any of the following:
- Identifying and treating the underlying cause of the problem
- Restricting fluid intake
- Taking medicines to help control potassium level in the blood
- Medicines taken by mouth or through an IV to help remove fluid from the body
Temporary dialysis can remove excess waste and fluids. This can help improve your symptoms so that you feel better. It may also make kidney failure easier to control. Dialysis may not be necessary for all people, but is often lifesaving, especially if potassium is dangerously high.
Potassium
This test measures the amount of potassium in the fluid portion (serum) of the blood. Potassium (K+) helps nerves and muscles communicate. It also ...

Dialysis may be needed in the following cases:
- Decreased mental status
- Fluid overload
- Increased potassium level
-
Pericarditis
Pericarditis
Pericarditis is a condition in which the sac-like covering around the heart (pericardium) becomes inflamed.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Removal of toxins that are dangerous to the kidneys
- Total lack of urine production
- Uncontrolled buildup of nitrogen waste products
Outlook (Prognosis)
ATN can last for a few days to 6 weeks or more. This may be followed by 1 or 2 days of making an unusually large amount of urine as the kidneys recover. Kidney function often returns to normal, but there may be other serious problems and complications.
When to Contact a Medical Professional
Call your provider if your urine output decreases or stops, or if you develop other symptoms of ATN.
Prevention
Promptly treating conditions that can lead to decreased blood flow as well as decreased oxygen to the kidneys can reduce the risk for ATN.
Blood transfusions are crossmatched to reduce the risk of incompatibility reactions.
Diabetes, liver disorders, and heart problems need to be managed well to reduce the risk for ATN.
If you know you're taking medicine that can injure your kidneys, ask your provider about having your blood level of the medicine checked regularly.
Drink a lot of fluids after having any contrast dyes to allow them to be removed from the body and reduce the risk for kidney damage.
References
Molitoris BA, Sharfuddin A. Pathophysiology of acute kidney injury. In: Alpern RJ, Moe OW, Caplan MJ, eds. Seldin and Giebisch's The Kidney . 5th ed. Philadelphia, PA: Elsevier; 2013:chap 76.
Turner JM, Coca SG. Acute tubular injury and acute tubular necrosis. In: Gilbert SJ, Weiner DE, eds. National Kidney Foundation Primer on Kidney Diseases . 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:chap 34.
-
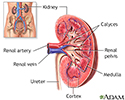
Kidney anatomy - illustration
The kidneys are responsible for removing wastes from the body, regulating electrolyte balance and blood pressure, and stimulating red blood cell production.
Kidney anatomy
illustration
-
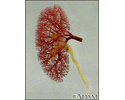
Kidney - blood and urine flow - illustration
This is the typical appearance of the blood vessels (vasculature) and urine flow pattern in the kidney. The blood vessels are shown in red and the urine flow pattern in yellow.
Kidney - blood and urine flow
illustration
-
Kidney anatomy - illustration
The kidneys are responsible for removing wastes from the body, regulating electrolyte balance and blood pressure, and stimulating red blood cell production.
Kidney anatomy
illustration
-
Kidney - blood and urine flow - illustration
This is the typical appearance of the blood vessels (vasculature) and urine flow pattern in the kidney. The blood vessels are shown in red and the urine flow pattern in yellow.
Kidney - blood and urine flow
illustration
Review Date: 9/22/2015
Reviewed By: Charles Silberberg, DO, private practice specializing in nephrology, affiliated with New York Medical College, Division of Nephrology, Valhalla, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Isla Ogilvie, PhD, and the A.D.A.M. Editorial team.